 Debbie Young
Debbie Young
By Debbie Young, MSL, ICCE, ICBD, ICPD, IAT, LCCE, CLC
Teaching about childbirth is a powerful opportunity to help future parents understand their options, build confidence, and navigate healthcare conversations with more ease. One topic that often raises questions—and sometimes anxiety—is labor induction. As educators who may not have a medical degree, we can still offer clarity, terminology, and context without providing clinical advice.
Labor is triggered by a complex, coordinated change in hormones that turns the uterus from a quiet, protective, and stretching muscle into a highly active, contracting one. The process is primarily driven by a “switching off” of pregnancy maintaining hormones like progesterone and a “switching on” of labor supporting hormones including estrogen, oxytocin, and prostaglandins. The human body generally works best when left to its own devices unless there is a medical need to intervene.
The rate of induction has risen significantly from 2018 to 2022 and possibly higher since that study (Nicholson et al., 2024). This guide explores how to explain induction in the classroom, when it may be medically recommended, when it may be optional, and how to inform students in a balanced, non-alarming, and non‑clinical way.
How to Explain the Process of Induction as a Childbirth Educator
When teaching induction, your role is to:
- Define the concept
- Explain common, nontechnical methods
- Describe the general purpose
- Avoid discussing specific medical recommendations or instructions
A classroom appropriate definition:
Labor induction means starting labor with medical help when it hasn’t begun on its own. Healthcare providers may use medicines or physical methods to help prepare the cervix and to start contractions. With induction, labor begins begins in a controlled setting where both the parent and baby can be closely monitored for safety.
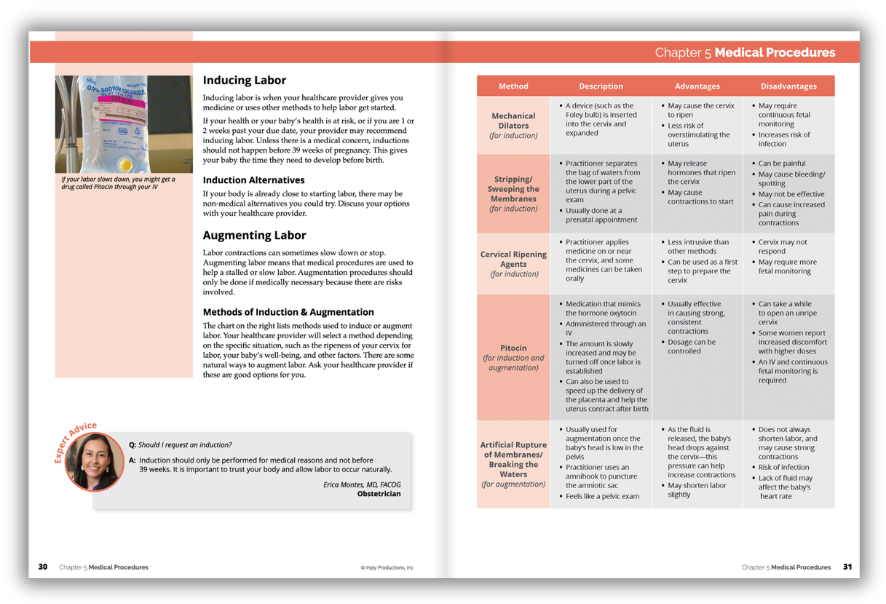
You can describe common methods without providing medical instruction:
- Cervical ripening: helping the cervix soften and thin.
- Medications: used to start contractions.
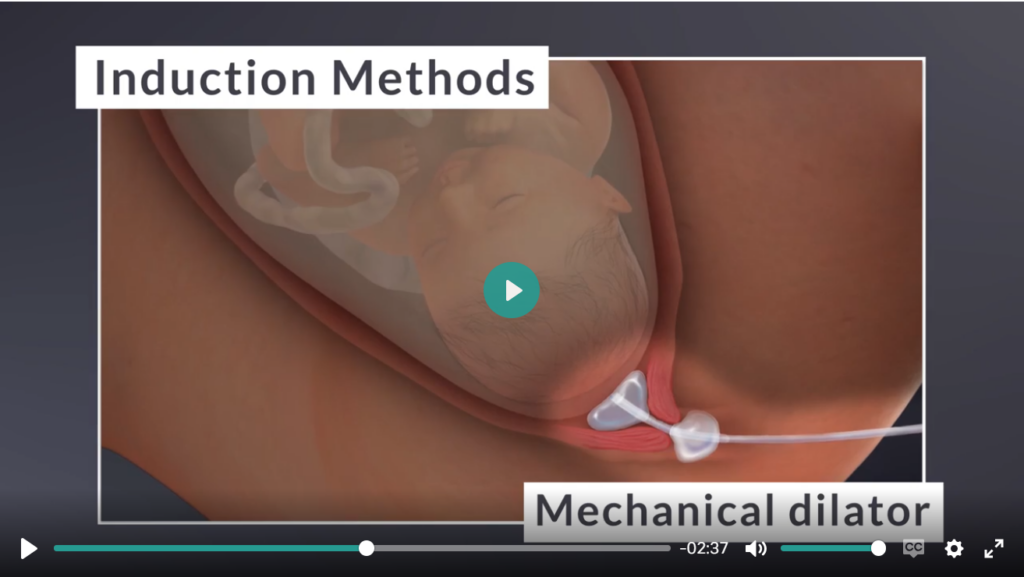
- Mechanical methods: such as a balloon catheter that gently encourages the cervix to open.
- Membrane sweep: a physical technique performed during an exam by a provider.
Keep the focus on concepts rather than procedures.
How to Explain When Induction May Be Necessary, Without Giving Medical Advice
Rather than discussing decision-making or clinical thresholds here, educators can list common reasons a healthcare provider might recommend induction. This helps students understand context without stepping outside of your role.
Examples include:
- Pregnancy going significantly past the due date
- Concerns about the mother’s health (for example, high blood pressure disorders)
- Concerns about fetal health or development
- Water breaking without labor beginning in a timely manner
- Infections or medical complications that make earlier delivery safer
Present these as “situations where a provider may discuss induction”—not as advice.

When Induction Might Be Optional or Elective
Sometimes induction may be a choice, not a requirement.
A helpful way to frame it:
Some individuals may be offered an induction for personal, logistical, or comfort reasons when they are already near term and healthy. This is typically called elective induction. Healthcare providers decide if someone is a good candidate and discuss risks and benefits.
Examples of elective contexts may include:
- Wanting to avoid going far past the due date
- Coordinating around partner or family availability
- Having a history of fast labors and living far from the birth location
Again, the key is to describe the concept, not recommend a specific choice.
How to Inform Without Causing Alarm
Induction can sound intimidating to learners who have never experienced or witnessed birth. Your goal is to explain the concept, emphasize the range of experiences, and highlight the role of supportive healthcare conversations.
Helpful teaching approaches:
- Use calm, neutral language.
Avoid emotionally charged terms like “force,” “danger,” or “failure.” - Acknowledge that induction is common.
Many births involve some form of induction, and outcomes are generally positive. - Present it as one of many birth pathways.
Not better, not worse—just another approach depending on circumstances. - Encourage students to ask their providers questions.
This builds confidence and reduces fear. (See B.R.A.I.N. ideas below)
A supportive framing might be:
“Induction is one tool that providers can use to help labor begin. Some people go into labor on their own, some don’t, and both can lead to healthy births.”
Understanding the Bishop Score and the Body’s Natural Preparation for Labor
When discussing induction, it can be useful to also explain the Bishop Score—a tool healthcare providers use to assess how ready the cervix appears for labor. This helps learners understand why inductions may differ in timing or approach.
What the Bishop Score Is
The Bishop Score is a scoring system used to describe cervical readiness. It evaluates:
- Cervical softness (firm, moderately soft, or soft/pliable)
- Dilation (how open it is)
- Effacement (how thinned it is)
- Baby’s station (how low the baby’s head is)
- Cervical position (facing the rear or front of body)
A higher score generally suggests the body appears closer to going into labor on its own. A lower score simply means the cervix may need more time or support to prepare.
As educators, the goal is to explain the concept, not to interpret scores.
How the Body Naturally Prepares for Labor
Even without induction, the body gradually prepares for labor through several key changes:
1. Cervical Ripening
Hormonal shifts soften and make the cervix more flexible in the weeks leading up to labor.
2. Effacement and Dilation
The cervix thins (effaces) and begins to open (dilate), sometimes long before active labor begins.
3. Baby’s Descent
The baby often settles lower into the pelvis, a process called engagement.
4. Increasing Uterine Activity
People may notice:
- Braxton Hicks contractions
- Cramping
- Back pressure
- Pelvic heaviness
These are normal signs of preparation.

Hormonal Coordination
A complex interplay of hormones between the mother, the placenta, and the baby most likely initiates the onset of labor.
How the Body Gradually Becomes Ready for Labor: Understanding Receptor Sites and Oxytocin
Understanding these natural processes helps students recognize that the body prepares for labor gradually, and that every mother’s readiness can vary widely.
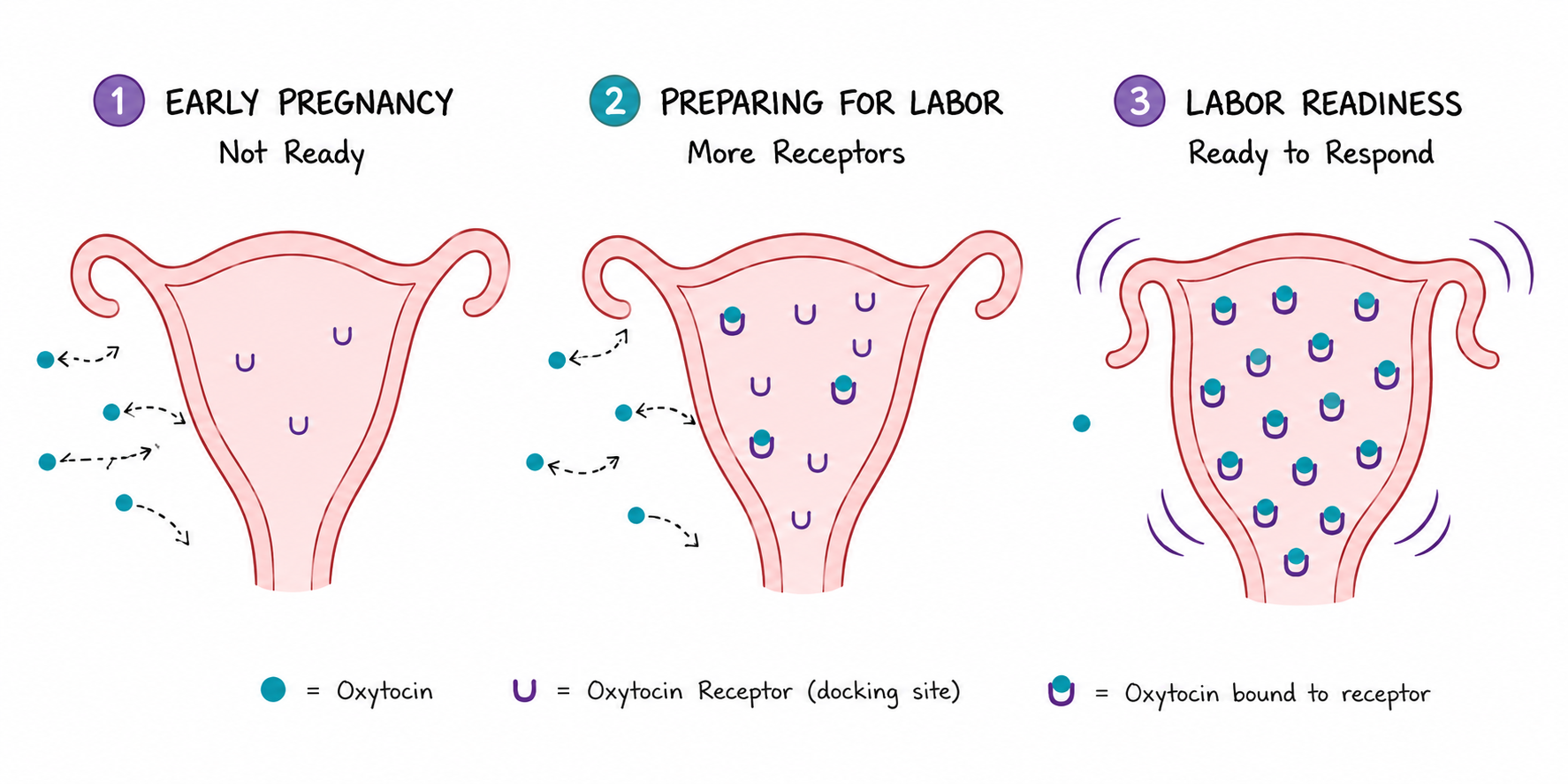
When teaching this concept, I often draw a simple uterus on the board and use it to explain oxytocin receptor sites. Oxytocin is one of the key hormones involved in labor, but the uterus can only respond to it when enough receptor sites are available.
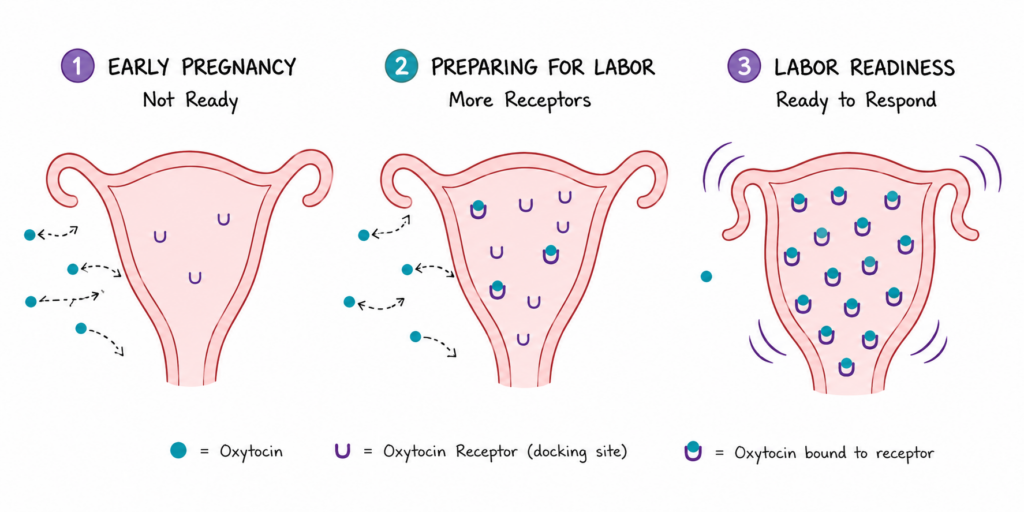
Early and Mid–Pregnancy: Few Receptor Sites
In the second trimester, the uterus has very few oxytocin receptor sites. Because of this, a mother may have only an occasional contraction when she engages in activities that naturally increase oxytocin, such as:
- Taking a long walk
- Having physical affection or intimacy with her partner (even kissing can boost oxytocin)
- Receiving a relaxing full body massage
These activities are considered normal and generally encouraged for healthy mothers without a history or risk of pre‑term labor.
If oxytocin is released during these moments, it may bind to one of the few available receptor sites, causing a light contraction. But because so many receptor sites are still closed or inactive, most of the oxytocin essentially “bounces off,” resulting in only mild, irregular tightening—more like gentle exercise for the uterus than true labor.
Approaching Full Term: Increasing Receptor Sites
As the body prepares for birth, the number of oxytocin receptor sites gradually increases. When I teach this, I draw additional receptor sites on the uterus to show how the body becomes more responsive over time.
With more open receptor sites, more oxytocin can “land” instead of bouncing off. This leads to:
- Stronger contractions
- More coordinated contraction patterns
- Cervical change
- The uterus responding more consistently
This visualization helps students understand why late pregnancy contractions feel different from earlier ones. It also helps students understand the chance of an induction leading to a successful lower intervention birth when mother’s body is ready but if it is not ready, it may take some time.
When Mother and Baby Are Both Ready
When both the mother’s body and the baby are ready for birth, the increase in receptor sites and the natural release of oxytocin work together beautifully. The result is a coordinated onset of labor that unfolds as the body was designed to function.
This demonstration reassures students that labor readiness is a gradual, hormonal process, not something that happens on a strict schedule—and that each body follows its own timeline. And also, induction is most likely to be successful when it is medically needed.
How to Teach About Induction Without Stepping Outside the Non-Medical Scope
As educators, it’s essential to avoid offering medical advice. You can teach how to communicate, what to ask, and what various terms mean—without suggesting specific decisions.
You can teach:
- Definitions and general concepts
- Questions patients might ask their provider
- Typical experiences or variations
- Emotional preparation
- Rights and shared decision-making
- Communication skills
- Evidence-informed childbirth education principles
What to avoid:
- Advising someone to choose or decline induction
- Discussing medical thresholds (“if your blood pressure is X…”)
- Recommending specific medications or methods
- Giving timelines or instructions
- Replacing provider guidance
- Interpreting or emphasizing specific research studies (e.g., the ARRIVE trial)*
*If parents are interested in research, guide them to reputable sources such as Henci’s Goer’s website and the Cochrane Library (opens in a new tab) where they can look at other research.
Useful, scope appropriate language:
- “Your provider may discuss…”
- “Some people experience…”
- “Ask your provider about…”
- “In many cases…”
- “One option that might be presented is…”
This keeps the conversation informational, not clinical. With that being said, you can always help them to use the B.R.A.I.N acronym to make sure they understand and have a choice in the matter.
Using the B.R.A.I.N. Acronym to Support Conversations About Induction
The B.R.A.I.N. acronym is a practical tool that helps mothers ask clear, focused questions when discussing induction with their providers. It encourages thoughtful decision making and supports respectful, two-way communication—without stepping into medical advice.
Below are induction-specific examples for each part of the acronym.
B — Benefits
What are the benefits of this recommendation?
Sample questions a mother may want to ask:
- What is the medical reason you’re recommending induction right now?”
- “How might induction benefit my baby?”
- “What benefits are there for me if we proceed with induction today or soon?”
- “Does my Bishop score suggest I’m likely to respond well to induction?”
R — Risks
What are the risks or downsides?
Helpful questions might include:
- “What are the possible risks to me or my baby if we choose induction?”
- “Are there risks if we wait for labor to start on its own?”
- “What are the potential side effects of the medications or methods used for induction?”
- “If induction doesn’t work, what would the next steps usually be?”
A — Alternatives
What other options are available?
Students can learn to ask things like:
- “If we don’t induce now, what are the safe alternatives?”
- “Could we monitor me and the baby more closely and decide later?”
- “Are there gentler or lower–intervention methods we could try first?”
- “Is membrane sweeping an option for me?”
I — Intuition
What does my own sense or instinct tell me?
Encourage mothers to reflect and ask:
- “Can you walk me through this again so I can process how I feel about it?”
- “This recommendation feels sudden to me—can we slow down and talk it through?”
- “Something doesn’t feel fully clear yet. Can you help me understand your concerns?”
This reminds students that intuition includes emotional readiness, comfort level, previous experiences, and how well they understand the information provided.
N — Not Now / No / Need More Information (Yes is also an appropriate answer if the parents want to move ahead)
Is it necessary to decide immediately? Is more information needed?
Depending on the situation, the “N” can be expressed in several ways. Sample questions include:
Not Now
- “Is it medically safe to wait an hour, a few hours, or even another day before deciding?”
- “What signs should we watch for if we postpone the induction?”
No
(When it is medically safe and the mother prefers to decline.)
- “If I choose not to be induced at this moment, how will we continue monitoring my baby and me?”
Need More Information
- “Can you show me my test results or explain what they mean?”
- “What numbers or findings specifically make you concerned?”
- “Can you explain how this recommendation fits with my overall health and pregnancy history?”
Conclusion
Teaching about labor induction doesn’t require medical credentials—it requires clarity, compassion, and respect for each family’s decision-making process. By explaining what induction is, when it may be used, how the body prepares naturally for labor, and how individuals can communicate effectively with their healthcare providers, you empower students without overstepping into medical territory.
Reference
Nicholson, S., Hatt, S., & colleagues. (2024). The rising tide: Trends in induction of labor at term over a 5‑year period at a single centre. International Journal of Gynecology & Obstetrics, 169(2), 383–390. https://doi.org/10.1002/ijgo.16054 (opens in a new tab)
Related Resource:
- InCast Season 10 Episode 1: The Induction Question: Evidence, Agency, and Informed Choice (opens in a new tab) with Henci Goer
Products Popular with Childbirth Educators:
- Understanding Birth Curriculum – Comprehensive teaching materials with interactive components
- Natural Birth & Beyond Video Library – Affordable On-Demand Video Library for Independent Educators
- The Miracle of Birth 3: Five Birth Stories (Video) – Engaging video content for classroom use
- The Stages of Labor 3rd Edition: A Visual Guide (Video) – Visual teaching tool for explaining labor progression


